A physical therapy exam typically includes an assessment of alignment, movement analysis, symptom modification procedures, range of motion, and muscle performance. But in the many exams you have likely performed, when was the last time you assessed speed?
When we think of speed, a picture of an elite sprinter frequently comes to mind. However, speed is essential not only for athletic performance, but also for injury prevention and treatment. Systematic reviews conducted by Menacho, et al., and Hoch, et al., suggest delays in peroneal muscle reaction time in participants with sprained ankles and chronic ankle instability, respectively.1, 2
Speed is also important to assess in patients at risk for falls. Think about the effect of gait speed on screening for fall risk during the Timed Up and Go test. For example, Tijsma, et al., found that choice stepping reaction time is slower in fallers compared to non-fallers in participants with multiple sclerosis.3
What Is Speed?
Speed is defined as the ability to move quickly across the ground or move limbs rapidly. It consists of four components:
1. Reaction time—the elapsed time between the presentation of a sensory stimulus and the subsequent behavioral response. This sensory stimulus can be either visual or auditory.
An auditory stimulus is a sound that causes a behavioral response. The average time to perform that action is 284 milliseconds.4
- Example 1: A baseball player starts to track a ball after hearing the “crack” indicating that it has been hit.
- Example 2: A pedestrian, who is looking at his phone, looks up in response to a cyclist saying “Hey!”
A visual stimulus is a visual cue that causes a behavioral response. The average time to perform that action is 331 milliseconds.4
- Example 1: A baseball player visually tracks a ball’s speed and path as it arcs across the field toward him.
- Example 2: A pedestrian moves to his right when he sees a cyclist quickly approaching him.
There are also two different forms of reaction time:
Simple reaction time occurs when there is one stimulus and a single response.
- Example 1: A sprinter runs straight ahead when hearing the starter gun go off.
- Example 2: An older adult steps to his right in response to a physical therapist clapping during a balance drill.
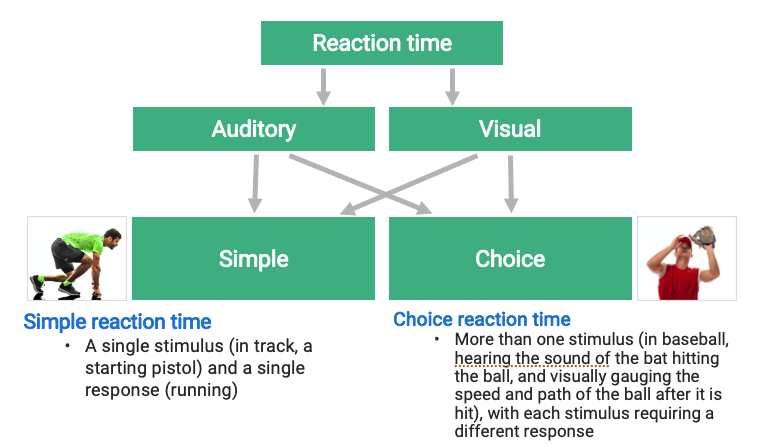
Choice reaction time occurs when there is more than one stimulus and each stimulus requires a different action.
- Example 1: A baseball player hears the sound of the ball being hit by the bat (auditory stimulus) and tracks the speed and path of the ball (visual stimulus) to adjust his positioning.
- Example 2: A pedestrian, who is looking at his phone, looks up in response to a cyclist saying “Hey!” (auditory stimulus) and tracks the speed and location of the cyclist (visual stimulus).
The graphic below shows how reaction time can be simple or choice with visual and/or auditory stimuli.
2. Acceleration—the rate of change of velocity in a given direction. It is essential for sports such as sprinting and other field or court sports.5
3. Maximum velocity—the maximum speed achieved in a given effort. Competitive athletes and elite sprinters can achieve this at 40 meters and 60 meters, respectively.
4. Speed Maintenance—the sustained maximal speed for as long as necessary. This becomes more important as running distances increase.6 This component of speed occurs from 40 to 60 meters and up to 200 meters.
Since maximum velocity requires at least 40 meters to achieve, most court and field athletes typically don’t achieve this. Volleyball courts are only 18 meters, and basketball courts are only 29 meters. Although soccer and football fields are 109 meters, the average sprint distance for soccer and football players is just under 6 meters.7, 8 This exemplifies the importance of reaction time and acceleration and suggests that maximum velocity and speed maintenance are rarely used in athletic performance.
In patients at risk for falls, improving reaction time is the most important component of speed to address. Therefore, we can improve performance and decrease fall risk by maximizing reaction time and acceleration.
Assessing Reaction Time
Simple visual reaction time can be tested with a ruler drop test. Hold a meter stick vertically above the participant’s hand with his or her thumb and index finger at the zero line without touching it. When the participant is ready, drop the ruler and have the participant catch the ruler as soon as possible.
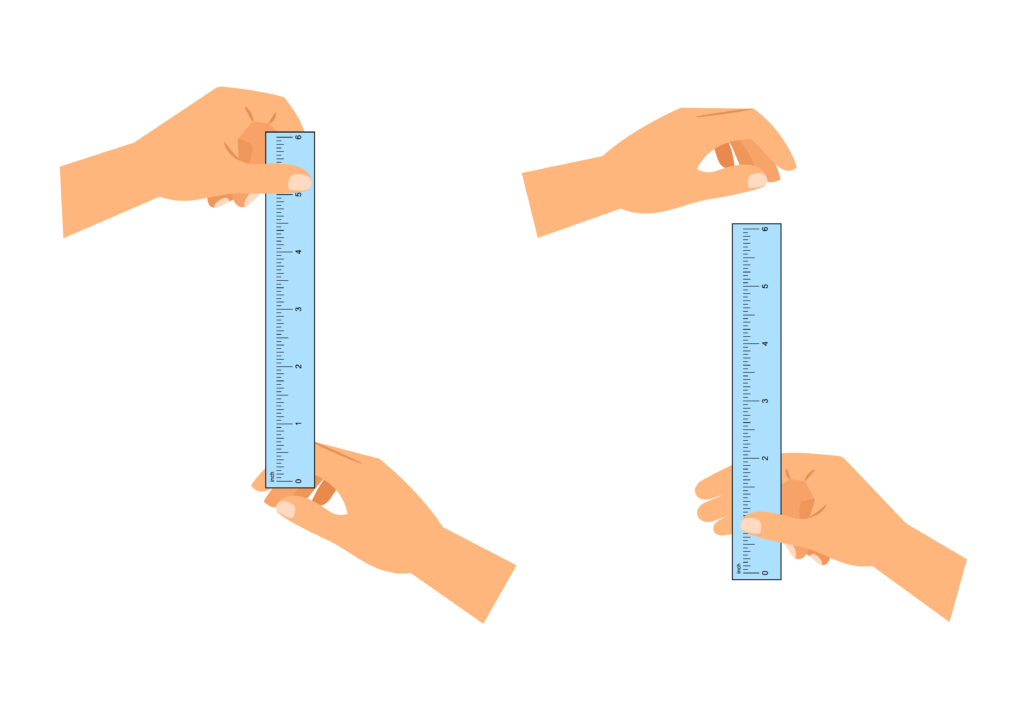
Perform several trials and take the average score. Reaction time can be calculated with the following equation,9 in which t is the time in seconds, d is the distance in meters, and g is the acceleration of gravity (9.8m/s2):
t = √ (2d/g)
Choice visual reaction time can be assessed as shown in the clip below.
Using a video recording app, you can look at the time codes when the paddle is turned and when the athlete makes a movement to calculate reaction time.
In a fall-risk population, you can assess choice step reaction time with a “low tech” setup as described by Delbaere, et al.10 To perform this test, set up a non-stick mat with measured out rectangles as shown below (measurements are in cm).
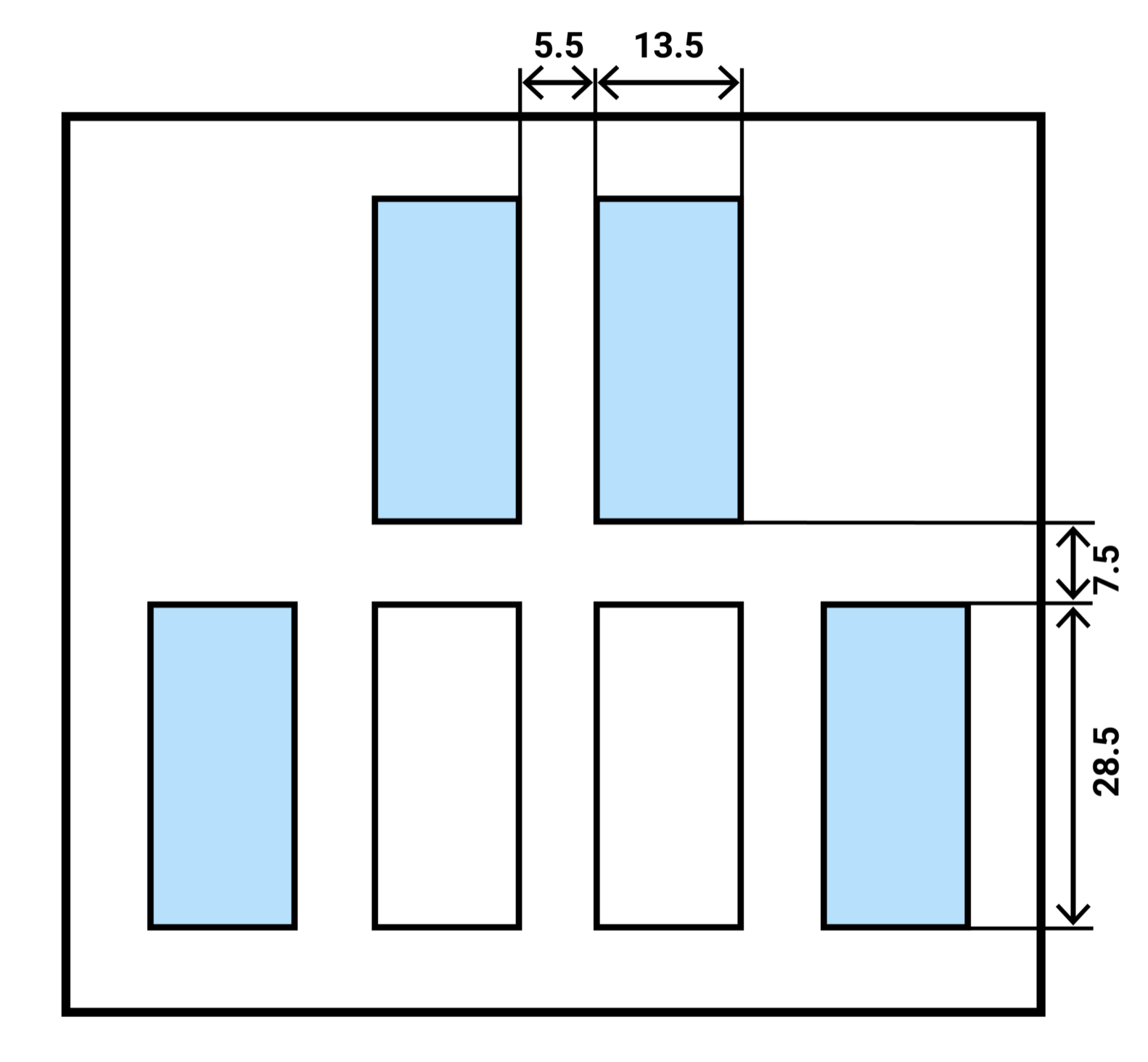
The middle white panels are considered the standing panels, and the blue panels are considered the stepping panels. The patient starts by standing with their feet in the standing panels, one foot in each panel. Instruct the patient to place their whole foot in one stepping panel and return to the respective standing panel. Next, instruct the patient to perform another step. The right foot should be used for the panels on the right side (both front and side), and the left foot for the panels on the left side.
State the instructions as, “front right,” “front left,” “side right,” or “side left.” Repeat for 20 trials and record the time. If the patient steps on the wrong panel or gets less than half of their foot in the rectangle, do not count that trial.10
Training Reaction Time
There are several ways to improve reaction time. Think about your athlete’s or patient’s goals and make it specific. For example, you could use tennis rapid-fire volleys, track starting drills, hopping on a compliant surface for ACL rehab, or catching a ball on a compliant surface for ankle sprain rehab. Be creative!
Take a look at this basketball-specific example:
In a fall-risk population, you can practice reactive and volitional stepping drills, which have been shown to reduce falls among older adults by approximately 50 percent.11 For example, you can train reactive stepping by attaching a sport cord around your patient’s waist, manually placing tension on it with your hand, and then releasing that tension. The patient must employ a stepping strategy to maintain balance. Just make sure that you are appropriately guarding the patient to protect them from falling if they misstep.
You can train volitional (choice) stepping by instructing the patient to step in a specific direction. For an increased challenge, you can hold up cards utilizing the Stroop effect, when the patient must follow the word instead of the symbol on a card.12
Testing Acceleration
In athletes, you can test acceleration time by performing a 20-meter sprint test and recording the time using apps that turn your smart phone into a “starter pistol” and your tablet into a time capture device. Using an app to time the start and finish is more accurate than timing it manually.
If you don’t have the space to perform a sprint test, you can assess an athlete’s movement performance and technique with a three-second wall sprint (shown in the video below), a movement that mimics the sprinting body position. Three seconds is ideal as that is approximately the average time it takes for elite athletes to accelerate.
Training Acceleration
Sprint acceleration can be trained with the wall sprints in three-second intervals while watching for hip flexion, knee flexion, and dorsiflexion. A similar drill can be performed with resistance, as shown below:
Speed is essential—not only for athletic performance, but also for daily life. Improving reaction time can help prevent falls in those at risk, and improving reaction time and acceleration can enhance athletic performance.
How else can you incorporate these concepts into your evaluation and treatment of your patients and clients?
Authors
About Jared Vagy, PT, DPT, OCS, CSCS

Dr. Vagy received his Doctorate in Physical Therapy (DPT) from the University of Southern California (USC). He has completed a one-year residency in orthopedics and a one-year fellowship in movement science. Dr. Vagy is a Clinical Assistant Professor of Physical Therapy in the DPT program at USC. He has published three books and numerous articles on injury prevention. Dr. Vagy delivers lectures and seminars internationally on the topic of The Movement System. He is an orthopedic clinical specialist and a certified strength and conditioning specialist.
Dr. Vagy has served as a physical therapist in China for the Chinese National Track and Field Team, worked with USA Track and Field at the Olympic Team Trials, completed a rotation at the US Olympic Training Center working primarily with USA Men’s gymnastics, and provided medical care at international events such as the International Weightlifting Federation World Championships. He has rehabilitated several world champions, gold medalists, and Olympic athletes. His assessments and treatments are rooted deeply in an understanding of The Movement System.
About Aimee Winston, PT, DPT

The original article and associated course can be found on the Medbridge blog page at this link: Click here